ℹ️ This is the case information for the doctor.
Name
Choe Williams
Age
7
Address
122 Stannard Close
Social history
7 year old attending Biddlestone Primary
Lives with maternal grandmother
Past history
Eczema
Investigation results
None
Medication
None
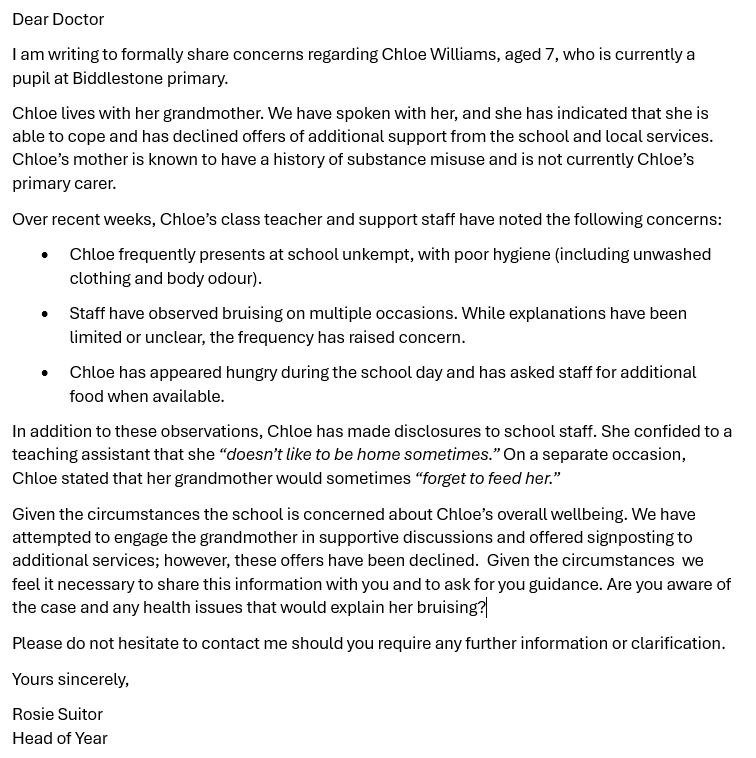
Booking note
Letter from school
ℹ️ This is the information for the person role playing the patient.
Name
Choe Williams
Age
7
Address
122 Stannard Close
Social history
7 year old attending Biddlestone Primary
Lives with maternal grandmother
Past history
Eczema
Medication
None
"What is this all about doctor, why have you called me in?"
ℹ️ To mark data gathering & diagnosis select from the descriptors below.
Positive descriptors
Negative descriptors
Data gathering was systematic and targeted ensuring patient safety.
Uses open questions to establish the concerns raised (e.g., asks grandmother’s concerns, daily life, Chloe’s routine, school attendance).
Progresses to targeted safeguarding questions about hygiene, nutrition, bruising, daily care, and gran’s capacity, without jumping to conclusions.
Data gathering was incomplete, lacking structure and focus.
Fails to explore the background or clarify the presenting issues; does not systematically ask about hygiene, supervision, and daily care.
Jumps to discussing safeguarding actions or legal rights before exploring the situation.
Makes effective use of existing information and considers the wider context.
Refers to the school report, highlighting specific concerns (attendance, bruises, poor hygiene, Chloe’s statements).
Investigates the background (mother’s history, household composition, previous social services involvement) and asks about past and current support.
Fails to use the information provided or understand the wider context.
Does not link concerns from the school letter to the consultation, relying only on the grandmother’s account.
Ignores or fails to gather contextual information about Chloe’s wider support system, living arrangements, or family dynamic.
The presence or absence of relevant red flags was established.
Checks for safeguarding red flags: unexplained or patterned bruising, missed meals, being left alone, poor hygiene, Chloe feeling cold/hungry, fears about home.
Asks directly if Chloe is ever unsupervised, about injuries, or if anyone has harmed or frightened her.
Fails to assess key information necessary to determine risk.
Does not ask about the specifics of bruising, possible supervision lapses, or instances of Chloe feeling unsafe or fearful at home.
Omits safeguarding screening when clear red flags are present.
Information gathered placed the problem in its psychosocial context.
Explores the impact of Chloe’s background (maternal substance misuse, separation from mother) and how both Chloe and grandmother are coping emotionally and practically.
Asks about family support, financial concerns, stress, and how gran manages her care role.
The social and psychological impact of the problem was not adequately determined.
Fails to ask how Chloe is coping with her family situation, separation from mother, or emotions about her home life.
Ignores the grandmother’s own stress, health, and support needs.
A working diagnosis was reached using a structured, evidence based approach.
Systematically builds a picture of possible neglect or safeguarding risk based on Chloe’s presentation, statements, and social situation.
Uses evidence from history and school report to consider differential (neglect vs. normal childhood accidents/difficulties).
The evidence collected was inadequate to support the conclusions reached.
Forms early conclusions (e.g. “It’s just clumsiness” or “Neglect is certain”) without gathering relevant, corroborative data.
Fails to distinguish between possible explanations or consider probability of safeguarding risk.
Uses an understanding of probability based on prevalence, incidence, and natural history to aid decision-making.
Recognises that, in this demographic, children in kinship care with history of parental adversity have higher risk of neglect.
Balances common childhood knocks with the significance of repeated, unexplained bruising/inadequate care.
Choice of data gathering does not reflect disease likelihood.
Overlooks the increased risk factors for children in Chloe’s position.
Fails to connect evidence of neglect with need for social care referral, or over-attributes benign explanations in face of multiple risk factors.
ℹ️ To mark clinical management & medical complexity select from the descriptors below.
Positive descriptors
Negative descriptors
Offers management options that are safe and appropriate
Explains to the grandmother that, due to the significant concerns raised, it is necessary to refer Chloe to children’s social services for further assessment, in line with safeguarding guidance.
Outlines that the priority is Chloe’s safety and that concerns around possible neglect and emotional harm require urgent and coordinated intervention.
Fails to provide appropriate and/or safe management choices
Does not raise the need for referral or downplays the severity of the safeguarding concerns.
Fails to take action to protect Chloe, or offers only to “monitor the situation” without escalating or involving appropriate agencies.
Continuity of care is prioritised
Arranges for clear follow-up: informs the grandmother about the next steps (e.g. social services will be in touch, Chloe will be seen by the safeguarding team).
Ensures that Chloe’s welfare is reviewed and that school and health professionals are kept in the loop regarding outcomes and ongoing risk.
Ongoing care is uncoordinated
Leaves the outcome uncertain, with no agreed follow-up plan or collaboration between agencies.
Does not communicate further steps to the grandmother or coordinate with school and social services.
Empowers self-care and independence
Provides empathetic support to the grandmother, offering advice and signposting to parental support resources, respite, or local help groups.
Encourages the grandmother to accept additional support where needed and reassures her that the aim is to enable her to care for Chloe safely.
Management fails to foster self-care and patient involvement
Offers little emotional support, allows the grandmother to feel blamed or abandoned, and fails to offer information or access to support networks.
Does not engage the grandmother in the management plan or explain available help.
Refers appropriately being mindful of resource
Makes a prompt, justified referral to children’s social services and, if necessary, the police (if immediate risk is suspected).
Liaises with school and safeguarding leads, ensuring all available information and concerns are shared to avoid duplicated or missed interventions.
Refers appropriately being mindful of resource
Fails to make a referral to children's services, or makes a referral without being explicit about the urgency of the referral.
Practises holistically, promoting health, and safeguarding
Recognises both Chloe’s vulnerabilities and the grandmother’s struggle; addresses wider needs, such as Chloe’s emotional well-being, practical support for the family, and health promotion.
Explores and addresses any broader risks, offers support for the grandmother, and facilitates access to resources.
Fails to safeguard patient welfare
Treats the concern purely as a social services matter, failing to engage with Chloe’s overall wellbeing or to support the carer.
Ignores wider risks for Chloe or the impact on the grandmother’s health.
Manages uncertainty, including that experienced by the patient
Discusses the uncertainty of Chloe’s situation and explains what will happen next with honesty and reassurance to the grandmother.
Clearly explains that a full assessment is needed, acknowledging that not all facts are clear, but emphasising a proactive and collaborative approach.
Struggles with uncertainty, leading to inconsistent decisions
Evades or deflects questions about the process, fails to acknowledge the distress and uncertainty faced by the family.
Gives unclear or conflicting messages about Chloe’s safety or what will happen next.
ℹ️ To mark relating to others select from the descriptors below.
Positive descriptors
Negative descriptors
Shows ability to communicate in a person-centred way:
Acknowledges Mrs Williams’ surprise and distress about the situation and the report.
Listens to her explanations about Chloe’s care, tackles her perceptions and emotions, and makes space for her to share her experiences.
Communication is doctor-centred and lacks empathy:
Focuses only on gathering facts or giving instructions, without exploring Mrs Williams’ feelings.
Misses her distress and anxiety about social services or being seen as a “bad” carer.
Treats patients fairly and with respect:
Shows respect for Mrs Williams as Chloe’s primary carer, addressing her worries non-judgementally whilst priortising Chloe's safety.
Avoids blame, recognises personal/cultural differences, and demonstrates compassion for her difficult role.
Decisions fail to prioritise the patient’s rights and interests:
Uses judgmental or accusatory language, making Mrs Williams feel blamed or stigmatised.
Ignores her right to be involved in discussions and is dismissive of her perspective.
Shows understanding of medical-legal principles and regulatory standards:
Explains the duty to safeguard children and why confidentiality may be overridden to protect Chloe.
Checks who has parental responsibility before discussing or sharing sensitive information, and clarifies the process.
Fails to give appropriate regard to key legal aspects of consulting:
Does not verify who holds legal guardianship for Chloe or what consent might be needed.
Omits to explain limits of confidentiality or fails to address these if Mrs Williams objects.
Recognises what matters to the patient and works collaboratively to enhance patient care:
Involves Mrs Williams in the discussion, makes it clear the child’s safety is the aim, not blame.
Negotiates a clear plan, making Mrs Williams feel part of the process rather than excluded.
Fails to work with the patient to plan care:
Proposes actions without seeking Mrs Williams’ views or acknowledging her input.
Makes unilateral decisions and creates barriers to cooperation.
Demonstrates flexibility of communication adapting to the patient and scenario:
Adapts language to avoid jargon and ensure Mrs Williams understands each step.
Clarifies and explains gently when discussing safeguarding, consent, or formal processes.
Consults rigidly, providing generic explanations and management plans:
Uses a fixed, process-heavy approach without making information accessible to Mrs Williams.
Does not check understanding or modify explanations when confusion or distress is evident.
Takes ownership of decisions, whilst being aware of personal limitations:
Makes clear, confident decisions about referral and safeguarding, while involving safeguarding leads as needed.
Explains personal responsibilities and willingness to consult other professionals for Chloe’s safety.
Does not take ownership or show awareness of personal limitations:
Defers all responsibility for safeguarding decisions to outside agencies, leaving Mrs Williams uncertain.
Fails to acknowledge own responsibility or role in the safeguarding process.
ℹ️ Insights from the examiner
Key Insight: The sequence of history-taking should be logical and responsive, following up cues given, and acknowledging each response.
Examples:
Key Insight: Demonstrate capacity to generate a differential that matches the safeguarding context (more than just ‘neglect’).
Example Differential:
Key Insight: Elicit how Chloe’s difficulties are impacting both her and her grandmother’s health, feelings, emotional wellbeing, and functioning.
Examples:
Key Insight: Explanations and risk communication should be clear, concise, and tailored to the carer’s concerns—avoid lengthy monologues.
Examples:
Key Insight: Make your reasoning transparent. Outline why you are taking each step, helping the grandmother understand safeguarding is about support.
Examples:
Key Insight: There’s a legal requirement to act. Provide options/support (as far as possible), focusing on transparency and collaboration.
Example Options:
Note: If grandmother refuses to consent, explain that by law you must share safeguarding concerns regardless of consent, but you will keep her informed.
References:
Key Insight: Personalise solutions: take into account the grandmother’s defences, exhaustion and reluctance, as well as Chloe’s emotions and risks.
Examples:



