16 years teaching experience for the RCGP consulting exams
💡 How can I reduce mistakes in my exams - the task bucket.
We were recently looking at JamesReason’s “Three Buckets”, a model that uses three categories (🪣self, 🪣context,🪣task) to assess the risk of making mistakes. The model can be used to recognise the causes of mistakes in the SCA exam. In the 3 buckets model the more items in your bucket the higher the risk of an error. So, to be ready for the exam we need to empty our buckets. Let’s look at the SCA task and the items that might fill an SCA Task bucket.
The task
Your SCA task is to complete twelve, twelve minute consultations covering a range of topics.
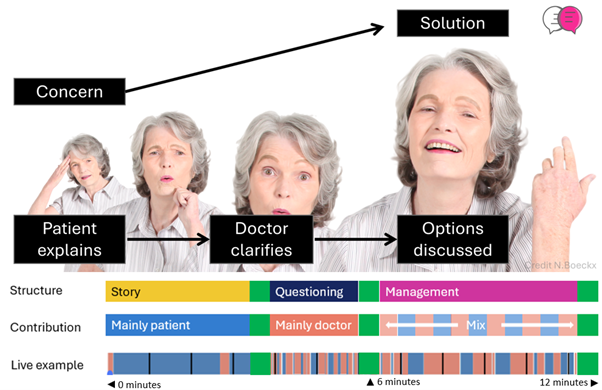
Your central goal in each case is to identify the patient’s concerns and provide a solution that addresses them.
To succeed in each case you must complete 3 sequential steps (1. explain, 2. clarify, 3. discuss)
1) Encourage the patient to explain their concerns
2) Clarify the patient’s issues using focused questions to complete the picture
3) Discuss the options as equals.
Strategies to “Empty” the Task Bucket
Story Strategies
Item
Impact
Strategy
🙁 Interrupts story → affects data gathering
Early interruption leads to missed cues and examiner perception of poor listening
🌟 Commit to open questions and an uninterrupted opening during the first 60–90 seconds.
🙁 Fails to understand the patient’s agenda
Agenda mismatch leads to unsafe or irrelevant management
🌟 Use an explicit agenda check by summarising your understanding to the patient.
🙁 Doesn’t connect to patient (knowledge, language, culture)
Examiner sees poor patient-centred care and reduced rapport
🌟 Echo the patient’s language, look for cultural cues, clarify technical terms, and regularly pause for questions.
🙁 Lacks curiosity and empathy
Consultation feels transactional; psychosocial drivers may be missed
🌟 Show you have understood the patient’s concerns in your replies and do not ignore patient comments.
🙁 Misses cues
Lost marks for interpersonal skills and data gathering
🌟 Adopt a cue-spotting habit: clarify emotional or vague statements before moving on.
🙁 Fails to manage expectations
Later conflict, dissatisfaction, or perceived unsafe care
🌟 Verbalise the patient’s expectations and how they are being addressed.
Questioning Strategies
Item
Impact
Strategy
🙁 Lacks logical question flow
Appears disorganised; increases omission risk
🌟 Connect your questions to the patient’s responses. Organise questions logically (e.g. red flags together, social questions together).
🙁 Working diagnosis doesn’t match story
Examiner perceives poor clinical reasoning
🌟 Create a differential diagnosis ordered by most probable cause and share it with the patient.
🙁 Forgets impact on home/work
Misses key information needed to understand the problem
🌟 Routinely ask about impact on daily life and work.
🙁 Questions/explanations are lengthy and confusing
Cognitive overload for patient and examiner
🌟 Aim for one clear idea per sentence. Keep sentences short and focused.
🙁 Misses key safety questions
Direct patient safety concerns
🌟 Routinely consider and verbalise red flags to ensure patient safety.
Management Strategies
Item
Impact
Strategy
🙁 Doesn’t explain thinking
Impaired consultation flow; reasoning for decisions or questions is unclear
🌟 Think out loud. For example: “I’m concerned about this chest pain, so I’d like to check your risk factors.”
🙁 Doesn’t provide a menu of options
Poor shared decision-making
🌟 Start management by offering options, guided by the patient’s preferences.
🙁 Doesn’t pause for patient involvement
Shared decision-making not demonstrated
🌟 Avoid monologues. Intentionally pause to invite patient engagement.
🙁 Gives generic solutions
Care is not individualised
🌟 Demonstrate how the patient’s preferences have been used to tailor management options.
Author
N. Boeckx
16 years teaching experience for the RCGP consulting exams
How much does it cost?
You may be entitled to free access through study budget because annual subscription is included in the Clinitalk course.